Originally published on the F.E.A.S.T Blog on August 22, 2014, by Lauren Muhlheim, Psy.D., CEDS, and Therese Waterhous, PhD/RDN
Eating Disorders are serious mental illnesses with dangerous medical consequences. Without early intervention, eating disorders may become chronic or even fatal. Parents are often unaware of some of the early signs of an eating disorder. Even if they are aware of early warning signs, they are often uncertain and reluctant to intervene out of fear of worsening the situation.
Family Based Treatment (FBT) is one of the leading evidence-based treatments for teens with eating disorders. Although not well-studied as an early intervention, one small study found that family-based early intervention for anorexia nervosa in teens is feasible and potentially beneficial.
![Early Intervention with Family-Based Treatment (FBT) for Eating Disorders [Image description: a teen girl sits next to a doctor who is writing notes; depicts a potential teen client with early signs of an eating disorder in California]](https://www.eatingdisordertherapyla.com/wp-content/uploads/2024/12/medium-shot-doctor-writing1.jpg "FBT Early Intervention | 93550 | 90255 | 95035 | 92553")
The Challenges of Early Eating Disorder Intervention
Eating disorders are notoriously hard to spot in the early phases. In the movie, Spotting the Tiger: Recognizing Early Signs of Anorexia in Children, narrated by Jamie Lee Curtis, she states, “Recognizing anorexia early is like trying to spot a tiger in the jungle. Trackers will tell you they never see the tiger, only the evidence of where it’s been. If you actually see the tiger, you are already in danger. The same is true of anorexia. When anorexia is obvious, serious damage has already been done.”
Once an eating disorder has fully developed parents usually look back with regret; they often identify numerous early warning signs that they missed. Because the signs are generally so subtle and, in many cases, look innocuous or even “healthy,” most parents are not prepared to intervene. Even pediatricians commonly advise parents to “watch and see what happens” before intervening. However, the development of an eating disorder is a slippery slope, and the situation can rapidly progress from mild to severe.
Potential Eating Disorder Warning Signs in Children and Teens
- Any weight loss in a growing child (even if the child was initially overweight) NOTE: Teens may lose weight for a variety of reasons; rule out other causes such as type 1 diabetes
- Dieting behavior or intention
- Rejection of foods or food groups previously enjoyed by a child or teen
- The child or teen skipping meals or saying they have already eaten
- Increased physical activity or movement (may not be goal-directed) in a teen or preteen not accompanied by increases in food consumption
- Failure to gain weight in a growing child or teen
- Slowing of the rate of gains in height
- Preoccupation with food preparation, recipes, or cooking shows
Children and Adolescents Who May Be At Increased Risk
Although we do not understand all of the risk factors for developing an eating disorder, the following are some factors that may increase an individual’s risk for developing one.
- Family history of anxiety-related disorders
- First-degree relative with a diagnosis of an eating disorder
- Traits of perfectionism
- History of anxiety
Two Case Studies of How FBT-trained Clinician Parents Used FBT for an Early Intervention
Case 1: Alexandra
“Alexandra” is the middle of three children, female age 11.5 at the time of the intervention. She has always been very active. Alexandra has always been a picky eater, especially about textural issues; for example, she has never liked crusts on bread, fat on meat, fried food, or potatoes. She is perfectionistic and competitive. She has tracked around the 50th percentile in weight for most of her childhood, slightly higher in height.
Specific warning signs and indicators for intervention:
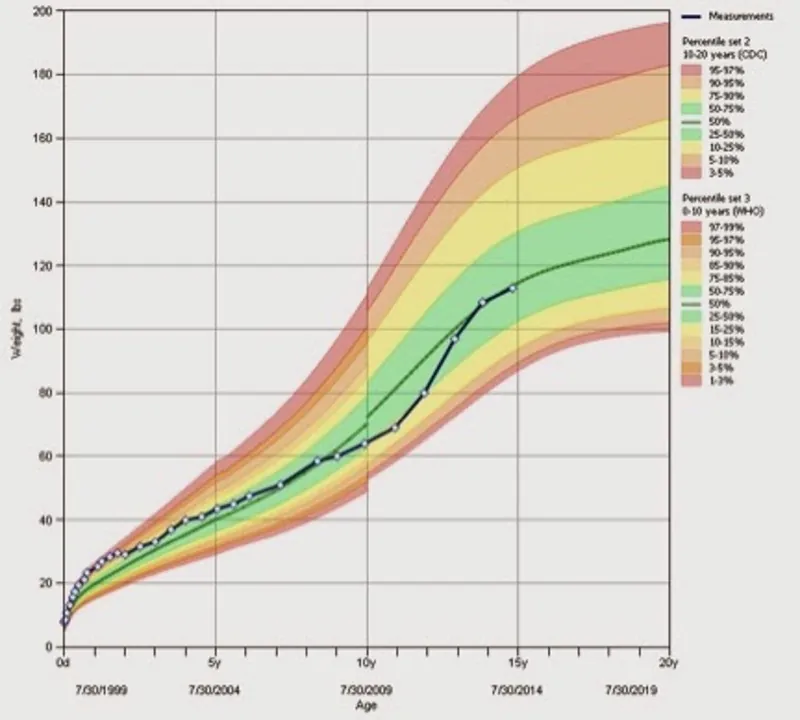
- Over the previous two years, Alexandra’s weight percentile had been slowly declining (from the 35th percentile down) while her height percentile was constant at 50%.
- Alexandra became extremely interested in food preparation, cooking, reading recipes, and watching cooking shows.
- Alexandra’s family moved home from an international assignment (a major stressor)
- Alexandra’s physical activity increased significantly as she progressed from recreation soccer to club soccer (the commitment increased from 2 days per week to 6 days per week). At the same time, her appetite and food consumption did not, on its own, increase.
- She did not ask for more food, but she also never expressed any dieting concerns or any concerns about shape or weight.
- On a day off school, Alexandra ran 2.5 miles, then stated she “felt great” immediately afterward. Following the run, she refused a meal of eggs (food she has never liked) and bacon (she proceeded to pick the fat off the turkey bacon because of complaints about the texture). She was content to eat nothing when she didn’t like the options available.
- However, she would eat foods such as desserts when offered
Parental interventions:
Parents agreed to do FBT early intervention with a focus on parents observing her eating during meals and helping her to eat enough to fuel for increased physical activity and growth.
![How we set recovery weights [Image description: Drawing of a doctor weighing a teen patient] depicts potential person with an eating disorder receiving therapy in Los Angeles, California](https://www.eatingdisordertherapyla.com/wp-content/uploads/2020/10/scale-final1-scaled.jpg "FBT as Early Intervention for Teen Eating Disorders | 90020 | 90010 | 90048 | 90210")
In the few situations where there was a predominance of foods she may never have eaten (due to the textural issue), parents offered alternatives to ensure she ate enough (distinct from the strategy parents used with the other children which was offering no alternatives to the primary meal in an effort to promote eating flexibility). Parents instituted regular weighings and spoke to her about their concerns.
Results
Over a four-month period during the intervention, Alexandra gained 6 pounds even as she joined a club soccer team and increased her physical activity. Eventually, her appetite did seem to “catch up” to her need, and her parents gradually reduced their oversight. The parents believe they helped Alexandra to keep up with her increased energy needs during this critical time period when she appeared unable–at least initially–to do so on her own. Anorexia nervosa can appear insidiously in situations like this (independent of any intention to diet or lose weight), so this early parental intervention is believed to have been effective based on FBT principles.
Over a two-year period, Alexandra gained about 18 pounds while growing 6.5 inches. Menarche occurred at age 13.5. At age 15, she is now fully back on her growth curve with height at the 75th percentile and weight at the 50th percentile. She eats normally and intuitively. It is notable that she no longer has a strong interest in cooking and cooking shows.
Case 2: Jack
“Jack” is a 15-year-old high school freshman who, at age 9 months, showed some early signs of food selectivity and avoidance of certain tastes and textures. He has never shown a large growth spurt but rather tracked along the same percentiles for much of his life. According to his parents, Jack has been a typical “kid eater,” preferring easy, bland, non-mixed foods and demonstrating food neophobia, typical in many toddlers and young children.
Growth charts show that from age 1 year until age 15 he was at 5th percentile for height and 10th to 25th for weight. Growth has been consistent, but the child’s pediatrician did order growth hormone levels measured, which showed a normal level of growth hormone. Jack was competitive but not overly perfectionistic, yet as Jack started high school he stated he wanted to achieve all A’s for all years of high school. His body type is muscular.
Specific Warning signs and indicators for intervention:
- During the previous year, Jack significantly increased physical activity participated in soccer conditioning camps, played JV soccer for high school, and recently joined a soccer club.
- Jack was not particularly interested in increasing food intake nor did he show greatly increased appetite.
- After 1 week of soccer conditioning, he showed a weight loss of 6 pounds.
- Jack has a full sibling diagnosed with anorexia nervosa at age 13, now recovered.
Parental intervention
Parents agreed to intervene by increasing caloric intake appropriately, taking weekly weighings, and providing guidance about the need to fuel increased
![Return to team sports during phase 2 of FBT [Image description: drawing of a teen boy playing soccer] Represents a potential teen with an eating disorder in counseling in Los Angeles, California](https://www.eatingdisordertherapyla.com/wp-content/uploads/2023/06/DALL·E-2023-06-08-20.13.30-a-drawing-of-a-teen-boy-wearing-a-purple-shirt-and-kicking-a-soccer-ball-on-a-field-viewed-from-behind1.png "Teen boy playing soccer | 90011 | 90650 | 91331 | 90201")
Jack did complain of feeling overly full on several occasions and his parents did not give in to the desire to allow decreased food intake. Parents increased his caloric intake by adding oils to foods such as pasta and rice, adding Instant Breakfast to milk, increasing portion sizes of meals, and requiring 2 snacks per day, minimum.
Results
Jack restored weight within 2 weeks. Weight monitoring continued through the freshman year of high school to ensure that Jack met the expected gains in weight and height. Over time, he maintained his weight and grew as expected according to lifetime growth charts. Gradually he was given more freedom to portion his foods, choose snacks, and have flexibility in terms of timing of snacks. Breakfast, lunch, and dinner were usually prepared and served family-style. Jack usually chose and prepared his snacks, a developmentally appropriate option when no eating disorder is present.
Two years later Jack has continued to develop normally, gaining expected height and weight. He eats a wider variety of foods and is less concerned about textures and new tastes. Given the positive family history of anorexia nervosa, it is especially appropriate to catch weight loss in a growing sibling early. Weight loss, whether intentional or not, is a significant trigger for the initiation of eating disorder pathology.
FBT Seemed Successful for Early Intervention/Prevention of Anorexia
These two situations may have been cases of anorexia averted. Certainly, there is no evidence that either child was harmed in any way by the parents taking charge of meals for a limited time.
![Family-based treatment for teen eating disorders in Los Angeles, California online or virtual [Photo description: drawing of a teen sitting at the dinner table and her parents are seated on either side. her brother and a dog are present. Her parents look very loving and supportive] Depicts a potential family receiving Family-Based Treatment in California](https://www.eatingdisordertherapyla.com/wp-content/uploads/2023/03/edfamilyFINALwatermarked-scaled.jpg "FBT as Early Eating Disorder Intervention")
We believe these case studies illustrate the great potential that FBT offers for early intervention.
Get Help For Your Teen With Early Signs of an Eating Disorder in California
You do not need to wait until symptoms are severe. Reach out to EDTLA if you are worried about your teen’s eating or exercise behaviors. Our caring eating disorder specialist therapists can help.
About the Authors
Lauren Muhlheim
Lauren Muhlheim, Psy.D., FAED, CEDS is a psychologist, fellow of the Academy for Eating Disorders (AED), and certified eating disorder specialist (CEDS) and approved supervisor for the International Association of Eating Disorder Professionals (IAEDP). She owns Eating Disorder Therapy LA in Los Angeles, CA. Dr. Muhlheim is the author of When Your Teen Has an Eating Disorder.
Dr. Muhlheim has held leadership roles in several professional organizations including the AED, IAEDP, and the Los Angeles County Psychological Association. She has previously been an IAEDP core course instructor and provides training on eating disorders to mental health providers internationally.
Therese Waterhous
Therese S. Waterhous PhD, RDN, CEDS-S, FAED is an eating disorder specialist in private practice in the Willamette Valley of Oregon. While no longer seeing patients, Therese remains active in teaching and training other healthcare professionals about eating disorders and advocating for those with eating disorders. As an advocate for those with eating disorders, Therese was one of the founding board members for the international non-profit advocacy group FEAST-ED (Families Empowered and Supporting Treatment for Eating Disorders). She delivers many local talks to various groups, educating them about eating disorders. In 2016-2017, she received and executed work on a grant from the local Coordinated Care Organization to train other healthcare professionals about eating disorder evaluation and treatment and extend eating disorder treatment to underserved Oregonians. She developed a state training for the Oregon Health Authority in 2021-2022 and is currently working on updating that training.
In the past, Therese served on the Oregon IAEDP (International Assn. for Eating Disorders Professionals) chapter board. Therese served on the Academy for Eating Disorders (AED) special interest group on Family-Based Treatment, the AED Medical Care Standards Committee and the AED Experts by Experience Committee. Currently, she serves AED on the Nutrition Task Force, the Clinical Standards of Care Committee, and the Special Interest Groups Oversight Committee.